

BACKGROUND
Bendamustine and Rituximab (BR) therapy is recommended in international consensus guidelines for treatment of Waldenström Macroglobulinaemia (WM) in both frontline and relapsed settings. The optimal dose and schedule of Bendamustine is not well established. Dose options include 90mg/m2 or 70mg/m2 on days 1&2 of each of 6 cycles (total Bendamustine dose of 1080mg/m2 and 840mg/m2, respectively) +/- reduction from 6 to 4 cycles.
AIMS
Determine response rates (IWWM criteria), PFS and toxicity following BR in frontline and relapsed settings
Determine the impact of depth of response and Bendamustine dose on PFS
METHODS
A multicentre, retrospective cohort analysis was undertaken of consecutive WM patients treated with BR in the frontline or relapsed settings. Data were collected from 17 sites across 4 countries, including UK centres participating in the Rory Morrison Registry.
RESULTS
Data from Sep 2010 to May 2020 were collected for 250 patients. Frontline (n=139, 55.6%) and relapsed (n=111, 44.4%) cohorts were matched in terms of sex, age at commencement of BR, ECOG score, and baseline parameters including: haemoglobin, platelet count, bone marrow infiltration, and presence of adenopathy, splenomegaly and extranodal disease.
At a median follow up of 37 months, disease progression had occurred in 25 frontline patients (18.0%) and 48 relapsed patients (43.2%; p<0.001). Death due to all causes had occurred in 16 frontline (11.5%) and 40 relapsed patients (36.0%; p<0.001).
Major responses (≥PR) differed significantly between frontline and relapsed cohorts (91.4% vs 73.9%, respectively; p<0.001), as did objective responses (≥MR; 97.8% vs 83.8%; p<0.001) and combined CR/VGPR rates (47.4% vs 24.3%; P<0.001). ECOG score, age and presence of extranodal disease were also predictors of response.
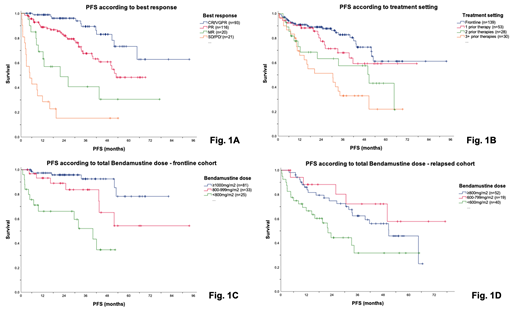
Best response significantly impacted on PFS and OS. Two-year predicted PFS rates for those achieving CR/VGPR vs PR were 96% vs 82%, respectively (p=0.002, Fig. 1A). Median OS was 83 months after achieving CR/VGPR, 65 months after achieving PR/MR and 28 months after achieving SD/PD (p<0.001).
Relapsed patients had received 1 (n=53, 47.7%), 2 (n=28, 25.2%) or ≥3 (n=30, 27.0%) prior therapies. PFS was significantly longer in the frontline cohort compared with recipients of ≥2 prior lines of treatment, but not between cohorts treated frontline vs after 1 prior therapy line (Fig. 1B). Rates of toxicity-related treatment truncation were significantly lower in the frontline setting (17.3% vs 35.1%; p<0.001).
Frontline patients received higher total Bendamustine doses than relapsed patients (median total dose 1080mg/m2 vs 720mg/m2; p<0.001), and dose was independently predictive of PFS. In the frontline setting, PFS was superior in the group receiving ≥1000mg/m2 (i.e. 90mg/m2 on days 1&2 for 6 cycles) compared with those receiving 800-999mg/m2 (p=0.04); two-year predicted PFS rates were 95% and 89%, respectively (Fig. 1C). In the relapsed cohort, by contrast, there was no PFS difference between the ≥800mg/m2 and the 600-799mg/m2 dose groups (p=0.19). Those who received doses of <600mg/m2 (i.e. ≤70mg/m2 on days 1&2 for 4 cycles, or less) had significantly poorer PFS outcomes compared with those who received ≥600mg/m2 (p=0.01), with two-year predicted PFS rates of 75% and 46%, respectively (Fig. 1D).
Age did not significantly affect tolerated dose in the frontline cohort, with similar median total Bendamustine doses in the <75-year and ≥75-year groups. Of note, 12/17 frontline patients aged ≥80 years received doses of ≥720mg/m2 (4-6 cycles with a starting dose of 90mg/m2). Older relapsed patients tolerated lower total Bendamustine doses: median dose received by subjects aged <65 years was 900mg/m2, compared with 720mg/m2 (65-74 years) and 540mg/m2(≥75 years).
CONCLUSION
Outcomes for WM patients following BR are excellent. Frontline patients tolerate higher doses of Bendamustine, and achieve deeper responses and longer PFS than relapsed patients. In both settings, attaining CR/VGPR results in superior PFS and OS. Our data clearly delineate the Bendamustine doses required to achieve optimum PFS. At frontline, 6 cycles of 90mg/m2 on days 1&2 is superior to lower doses with respect to response and PFS. In the relapsed cohort, maximum response and PFS benefit are seen with 4 cycles of 90mg/m2 on days 1&2; a starting dose of 70mg/m2 on days 1&2 is also sufficient provided 5-6 cycles are administered.
Menne:Kyowa Kirin: Other: Travel expenses; AstraZeneca: Research Funding; Pfizer: Honoraria, Other; Atara: Honoraria; Novartis: Honoraria, Research Funding; Kite/Gilead: Honoraria, Other: Travel expenses; Celgene: Honoraria, Other: Travel expenses; Daiichi Sankyo: Honoraria; Amgen: Honoraria, Other: Travel expenses; Janssen: Honoraria, Research Funding; Takeda: Honoraria; Bayer: Other: Travel expenses; Roche: Honoraria. Talaulikar:Janssen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Amgen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Roche: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Takeda: Research Funding. Pratt:Binding Site Ltd: Other: Personal fees; Amgen: Other: Personal fees; Janssen: Other: Personal fees; Celgene: Other: Personal fees; Takeda: Other: Personal fees; Gilead: Other: Personal fees; Sanofi-Genzyme: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Beigene: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Karyopharm: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding. Manos:Bristol-Myers Squibb: Other: Conference sponsorship. Gavriatopoulou:Genesis Pharma: Consultancy, Honoraria; Amgen: Consultancy, Honoraria; Janssen: Consultancy, Honoraria; Takeda: Consultancy, Honoraria; Karyopharm: Consultancy, Honoraria. Minnema:Kite, a Gilead Company: Speakers Bureau; Celgene: Other: travel support, Research Funding; Servier: Consultancy; Amgen: Consultancy. El-Sharkawi:Roche: Other: Conference fees; Janssen: Honoraria, Membership on an entity's Board of Directors or advisory committees. Kersten:Kite, a Gilead Company: Consultancy, Honoraria, Other: travel support; Novartis: Consultancy, Honoraria, Other: travel support; Miltenyi: Consultancy, Honoraria, Other: travel support; Roche: Research Funding; Takeda: Research Funding; Celgene: Research Funding. McCarthy:Abbvie: Membership on an entity's Board of Directors or advisory committees; Janssen: Honoraria. Bishton:Janssen: Consultancy; Takeda: Other: Travel/accommodations/expenses, Research Funding; Roche: Other: Travel/accommodations/expenses, Research Funding; Gilead: Other: Travel/accomodations/expenses, Research Funding; AbbVie: Research Funding. Follows:Roche: Consultancy, Other: Paid lecturing; Karyopharm: Consultancy, Other: Paid lecturing; Janssen: Consultancy, Other: Paid lecturing; Abbvie: Consultancy, Other: Paid lecturing; Bristol Myers Squibb: Consultancy, Other: Paid lecturing; Astrazeneca: Consultancy, Other: Paid lecturing. Wechalekar:Janssen, Takeda, Caelum, Celgene: Honoraria, Membership on an entity's Board of Directors or advisory committees. D'Sa:BeiGene: Honoraria, Research Funding; Janssen: Honoraria, Research Funding; Sanofi: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal